MEDICINE : Spotters

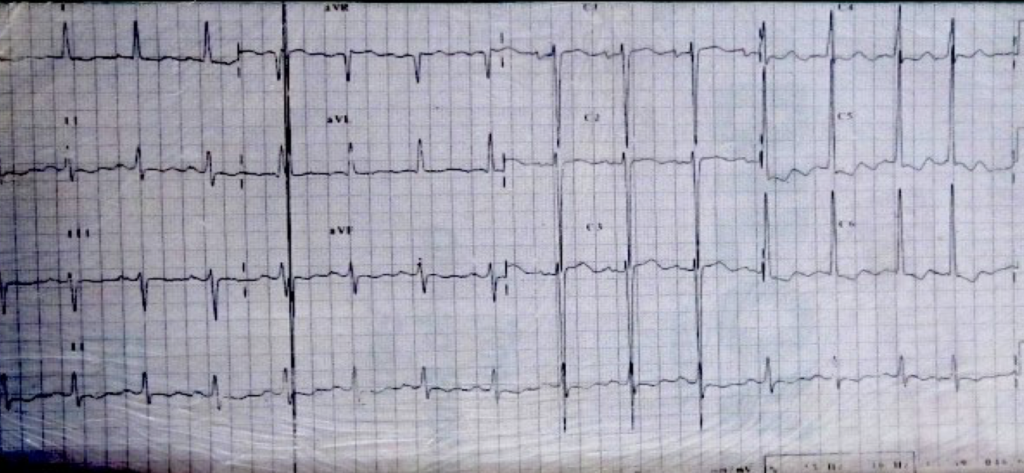
- Irregular R-R interval,
- Atrial fibrillation at a controlled ventricular rate 80/min
- absence of p waves, replaced by fibrillary waves,
- ST depression and T inversion at v5,6
- s at v1+ R in v6=42
- Dx= LVH with strain pattern, most likely systemic hypertension
Q. Mention 2 clinical findings
- AF- absence of ‘a’ waves in JVP
- LVH- apex shifted out and down, well sustained heave
Q. Modalities of t/t:
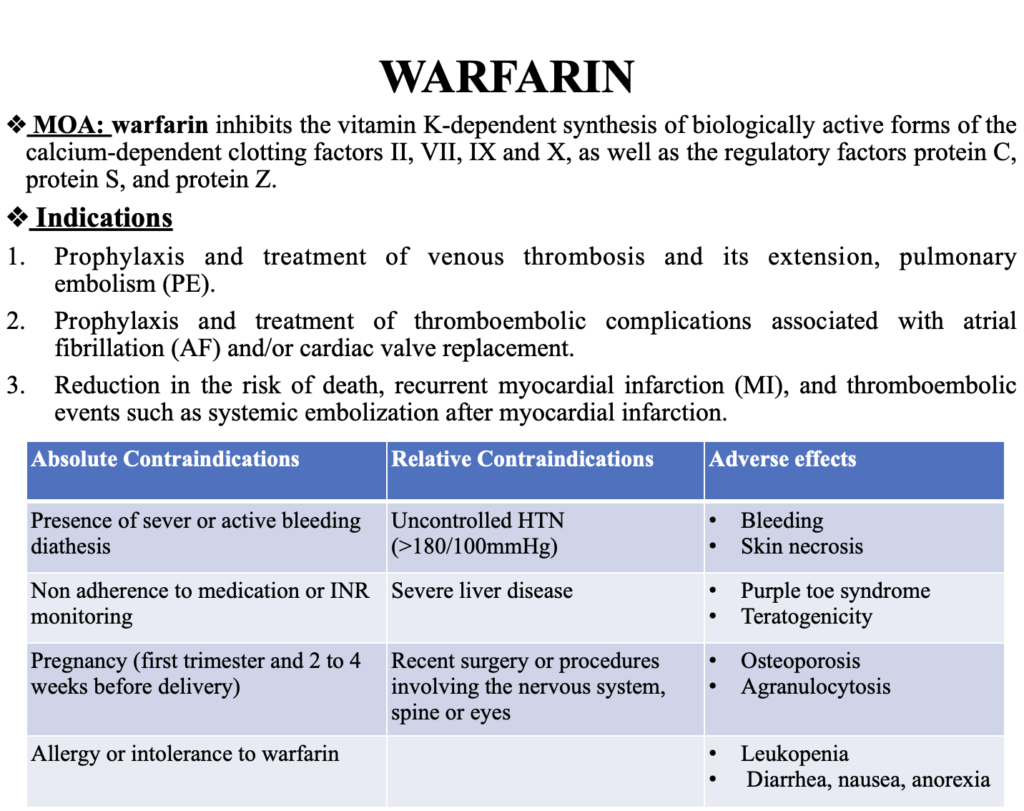
- Long term anticoagulant therapy
- Anti-hypertensives
Q. Complications:
Immediate- ventricular hypertrophy and Af- left sided heart failure
Long term- thromboembolism
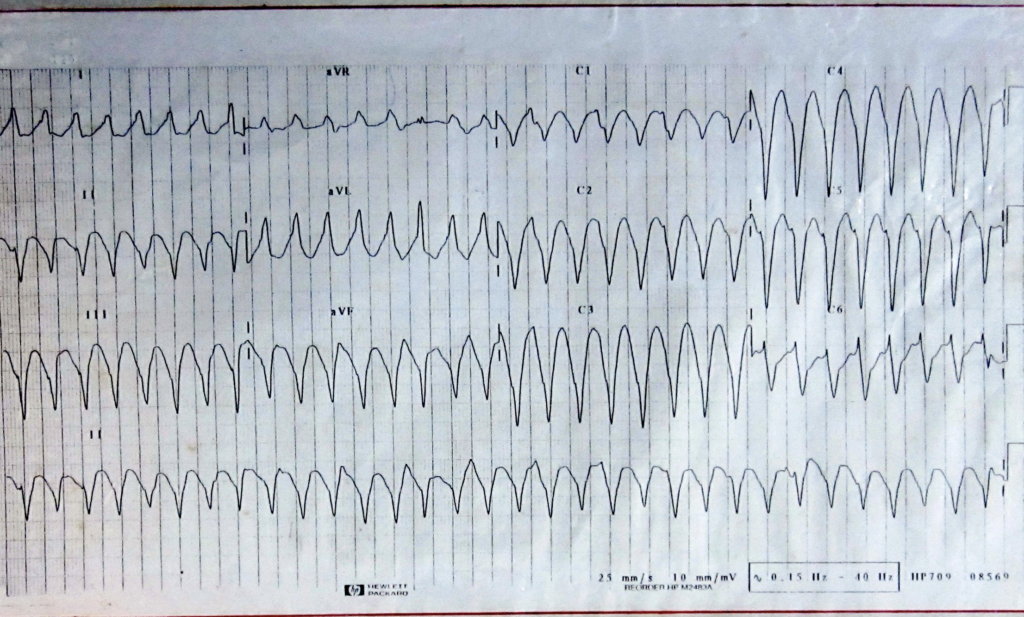
- Bizarre and Wide QRS, tachycardia rate 240/min,
- concordant QRS complexes in v1-v6,
- Evidence of atrial activity in between with a fusion beat
- Dx=ventricular tachycardia
Q. Mention two factors that cause this?
Ischemic heart disease
Cardiomyopathy
Electrolyte abnormalities (hypokalemia, hypomagnesemia)
Q. Two modalities of t/t
Immediate: DC shock 100-200J
Drugs: Amiodarone, Lidocaine
Q. Complications:
Sudden death
Cardiogenic shock
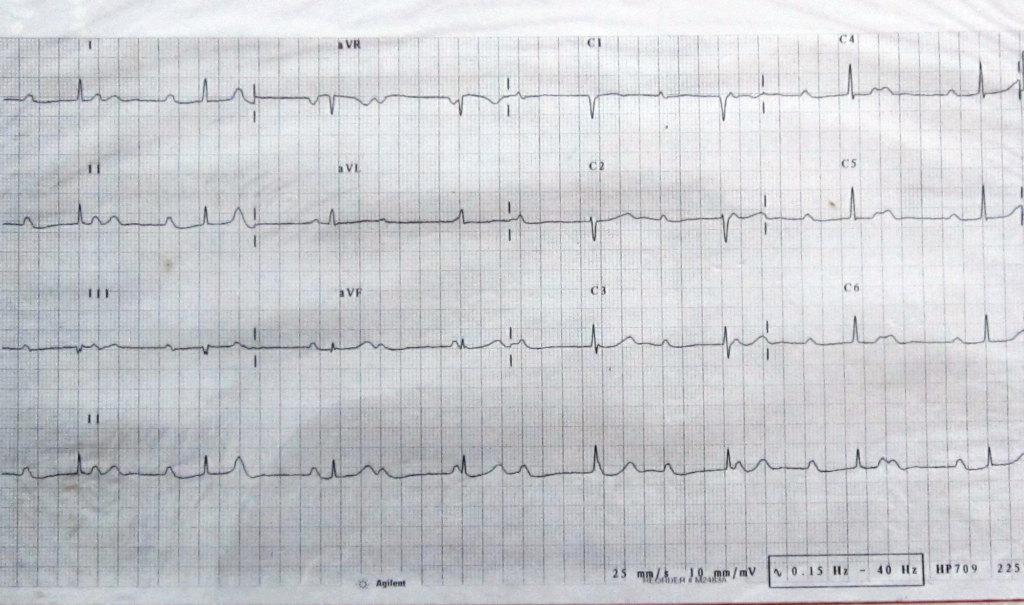
- Independent P and QRS complexes having no relationship,
- ventricular rate is 45/min
- Dx= complete heart block
Q. 2 Clinical features
Cannon waves in JVP
Variable intensity of S1
Q. 2 modalities of t/t
Permanent pacemaker
Isoprenaline

- ST elevation in lead II III AVF,
- reciprocal changes in I and AVL
- Abnormal Q wave in lead III (>20% of QRS complex)
- Dx= inferior wall MI
Q. How to confirm the diagnosis
Cardiac biomarkers
Echo
Q. Complications:
Various degrees of heart block
Right ventricular infarction
Q. T/t
Percutaneous angioplasty
Thrombolysis therapy (if no contraindications)
- ST elevation in lead II III AVF,
- reciprocal changes in I and AVL
- Abnormal Q wave in lead III (>20% of QRS complex)
- Dx= inferior wall MI
Q. 2 modalities of T/t
Carotid sinus massage
Valsalva maneuver
Drugs: Adenosine
Q. Likely ECG findings in this patient if in sinus rhythm?
Accelerated conduction (WPW syndrome)
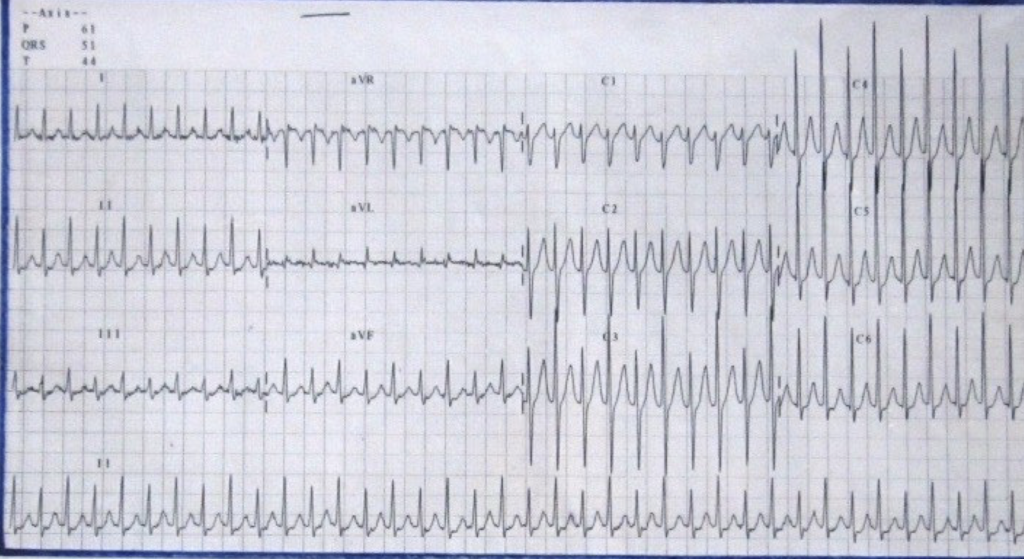
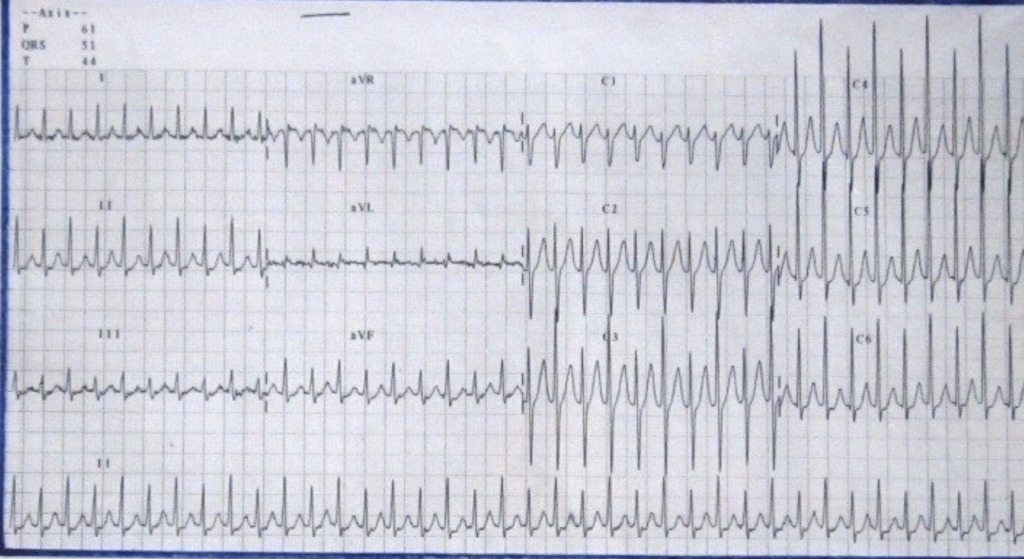
- Narrow QRS complexes coming at a regular interval of 250/min,
- absence of P waves
- Dx= PSVT
- additional findings- alternate QRS are tall and small-electrical alterans
Q. 2 modalities of T/t
Carotid sinus massage
Valsalva maneuver
Drugs: Adenosine
Q. Likely ECG findings in this patient if in sinus rhythm?
Accelerated conduction (WPW syndrome)

- Regular RR interval at a rate of 105/min
- Right axis deviation, incomplete bundle branch block
- Tall and peaked p waves in II III AVF = P pulmonale,
- QR waves in V1 and persistence of S waves in lateral chest leads (v5, v6)
- Dx= right atrial and Right ventrical hypertrophy most likely cor pulmonale
Q. 2 Clinical findings
Aunscultation: Loud P2
Early Diastolic murmur (Graham Steel murmur)
Q. 2 likely causes
COPD
Infarct of pulmonary artery
Q. 2 T/t modalities
- Long term O2 therapy
- Phlebotomy
- Regular RR interval at a rate of 90/min
- Left ward axis
- Broad & bifid P waves in lead 2,3 & AVF = p-mitrale
- SV1 + RV6 = 50mm
- ST depression in V5 & V6
- Dx = LVH with strain
Q. 2 likely causes
Systemic HTN
AS
Cardiomyopathy
Q. C/F
Apex beat shifted outwards and downwards
Well sustained heave

- ST elevation in V1 – V4, max at V3
- High take off of T waves .
- Tall & broad T waves.
- Hyperacute: No reciprocal changes, No Q waves
- Dx = hyperacute anterior wall myocardial infarction
Q. How to confirm the diagnosis
Cardiac biomarkers
Echo
Q. Complications:
Early- V tach, V-fib, huge pulmonary edema
Late- Dressler’s syndrome, Aneurysm of heart
Q. T/t
Percutaneous angioplasty
Thrombolysis therapy (if no contraindications)
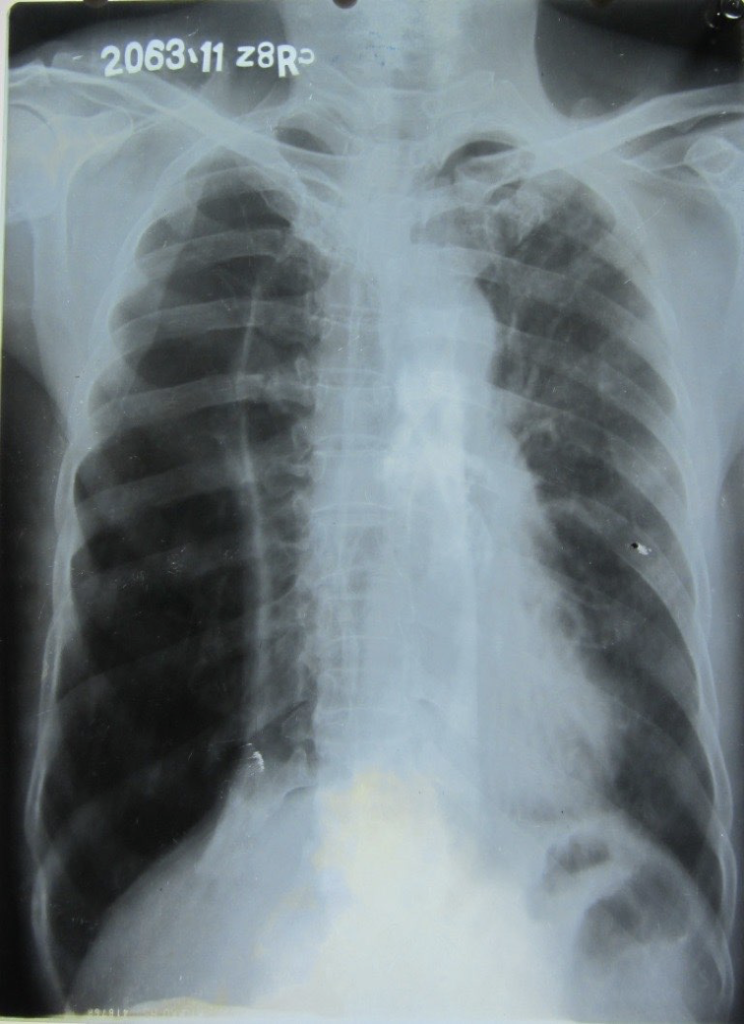
- Triangular homogenous opacity in right middle zone, sharply demarcated below by horizontal fissure
- Dx= Right upper lobe segmental consolidation
Q. 2 organisms
Pneumococcus, Staphylococcus
Strep.pneumoniae, H. influenza, Klebsiella, Chlamydia, Mycoplasma,
Q. 2 Complications
Parapneumonic effusions
DIC

- Low – 11 posterior ribs seen & flat diaphragm
- Ribs are wide & horizontal
- Tubular & elongated heart
- Giant bullae seen in right lower & left middle zone with compression of lungs
- Dx= emphysema with giant bullae
Q. 2 Likely clinical findings
Pursed lip breathing
Hyper-inflated lungs on percussion
Q. T/T
Bullectomy
Incentive spirometer
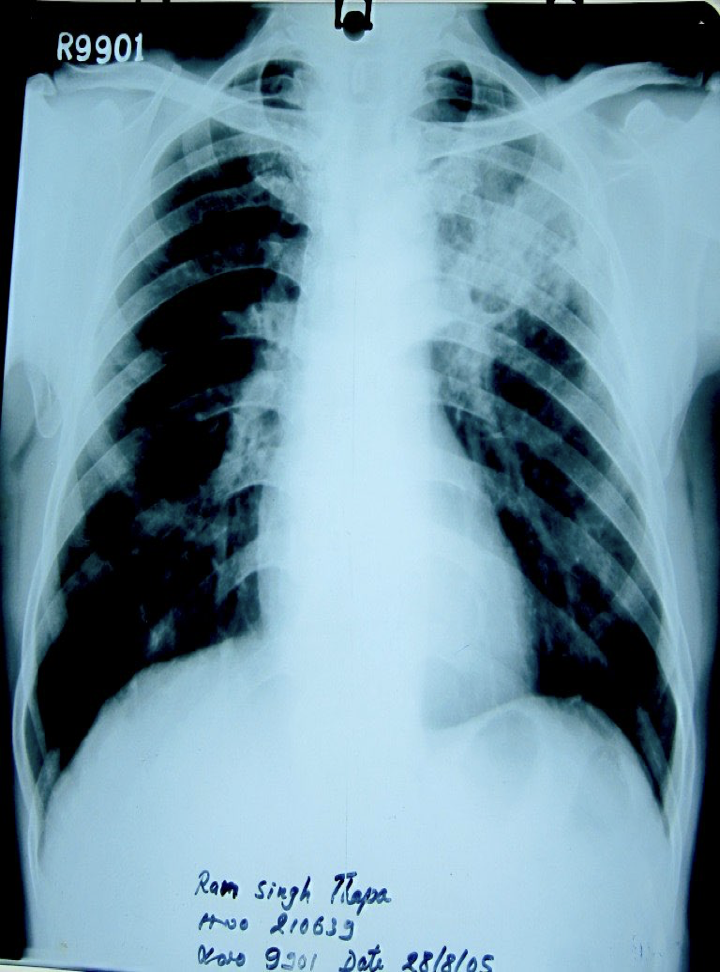
- Non homogenous opacity in left upper zone with fibrous bands
- Thin walled cavity/ abscess , no air-fluid levels
- Dx= post primary pulmonary TB with fibro cavitary lesions.
Q. Most likely complication
Aspergilloma
Q. T/T
Surgical removal/drainage
Q. Etiology of upper lobe abscess
TB
Klebsiella

- Cardiomegaly
- Straightening of left border of heart with enlarged left atrial appendage
- Shadow behind shadow seen on right side of heart
- Dilated upper lobe pulmonary veins both lung fields
- Dx= MITRAL STENOSIS
Q. Mention 2 C/F
- Mid-diastolic murmur…presystolic accentutation…(describe murmur)
- Opening snap
- Tapping apex beat
Q. Complications
Pulmonary hypertension
AF
IHD
Q. 2 modalities of T/T
Mitral valvulotomy
Valve replacement
Digitalis
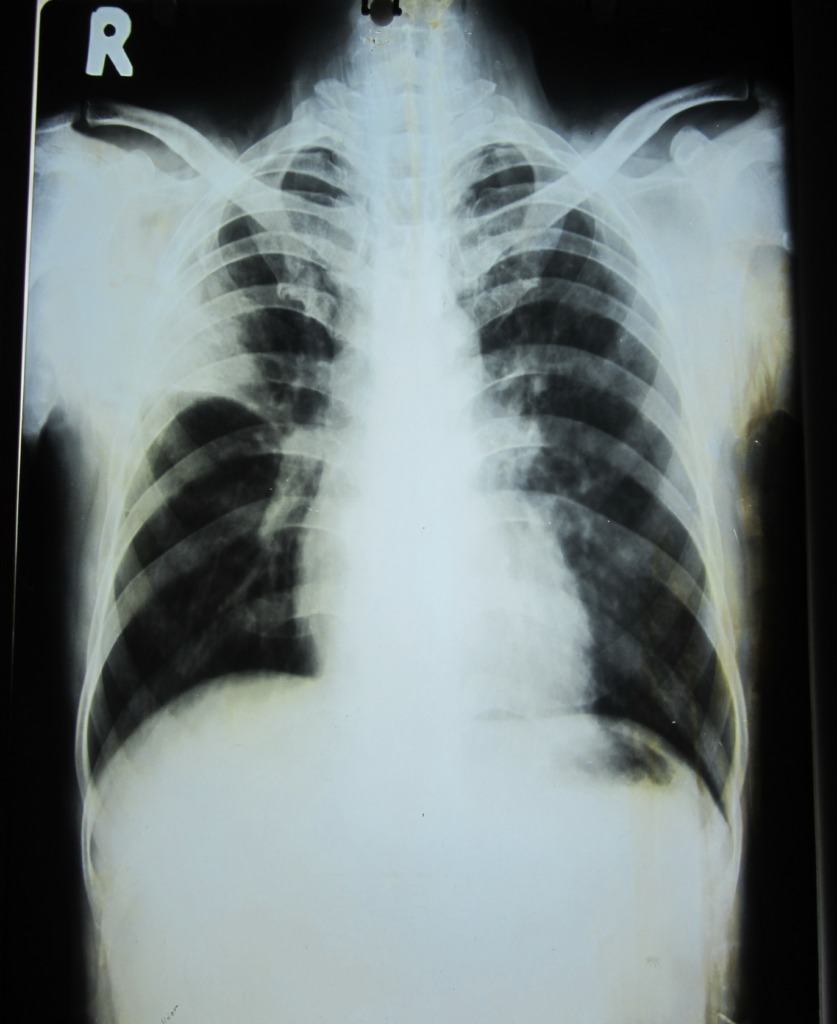
- Complete loss of lung markings in the outer 2/3 of right lung fields
- Collapsed lungs seen on right side
- Mediastinum shifted to left side
- Dx = right sided tension pneumothorax
Q. 2 modalities of T/T
- Needle aspiration at right second intercostal space in MCL
- Closure of the bronchopleural fistula
Q. 2 Etiology
Trauma
Emphysema
TB
Q. 2 C/F
Collapsed lung- Low Bp
Central cyanosis
Hyper resonant lung with absent breath sounds
- Cardiomegaly
- Straightening of left border of heart with enlargement of main pulmonary artery trunk
- Enlargement of right pulmonary artery
- Peripheral pruning of pulmonary artery
- No prominent pulmonary veins on upper lobe
- No double shadow on right heart border
- Dx = Pulmonary arterial hypertension with right ventricular hypertrophy
Q. 2 symptoms which she can develop later
Hoarseness of voice
Dysphagia
Hemoptysis

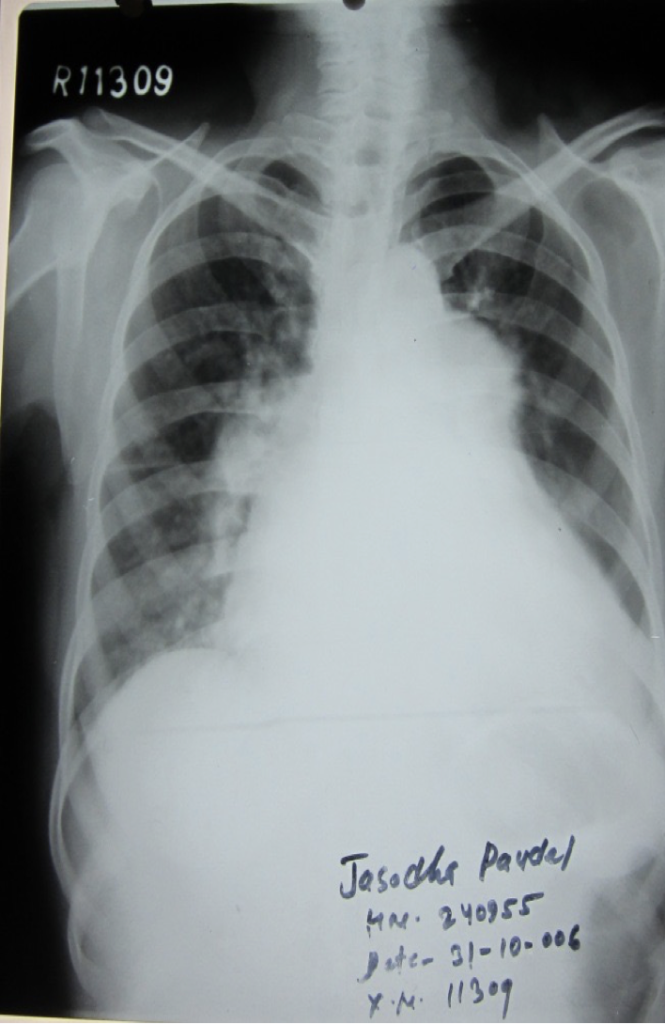
- Dense homogenous opacity in right lower zone
- Opacity goes extends in a straight line towards axilla
- Mediastinum shifted to right
- Right hemithorax smaller with crowding of ribs
- Evidence of loss of lung markings (translucency) on left lower zone
- Evidence of hyperinflation of lung on left lung- wide and horizontal ribs
- Dx = right sided pleural effusion with decreased lung volume on right side and compensatory emphysema on left side
right sided pleural effusion with decreased lung volume on right side and compensatory emphysema on left side
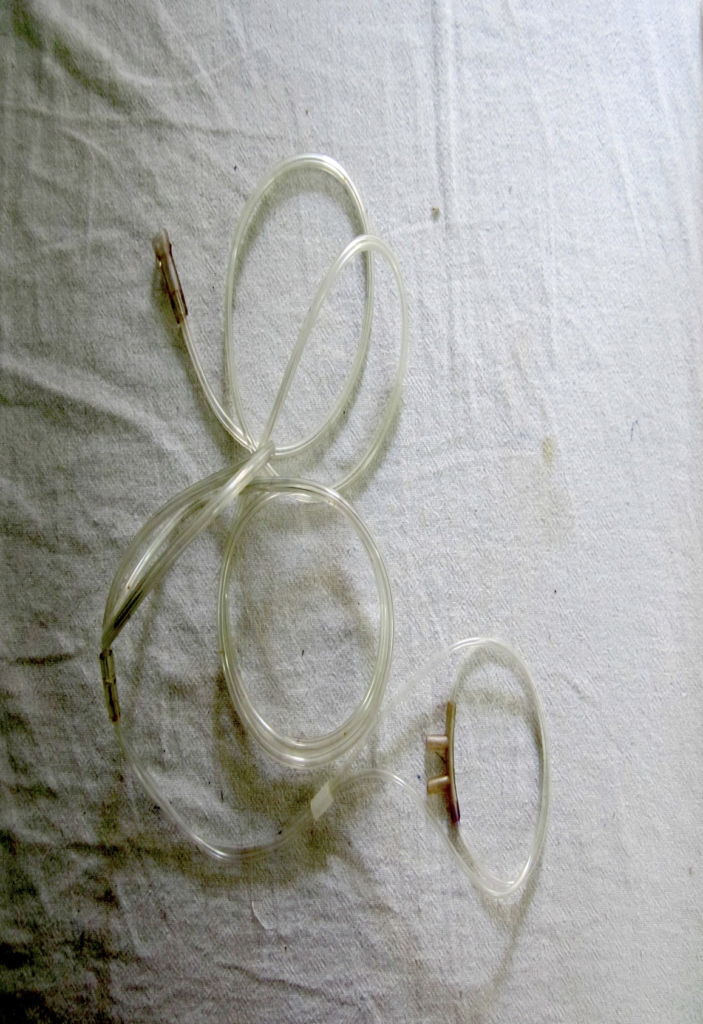
- Oxygen catheter
- Indications:
- Documented hypoxemia as evidenced by:
- PaO2 < 60 mmHg or SaO2 <90% on room air
- PaO2 or SaO2 below desirable range for a specific clinical situation
- Acute care situations in which hypoxemia is suspected (dyspnea, tachypnea, bradypnea, pallor, cyanosis, lethargy, use of accessory muscles of respiration
- Severe trauma
- Acute MI
- Pulmonary HTN
- Short term: Post anesthetic recovery
- Contraindications:
- Patient not giving consent
- Nasal obstruction
- Complications:
- Oxygen toxicity
- Oxidative stress
- Absoprtion atelectasis
- combustion

- Cuffed endotracheal tube
- Indications:
- Protection of airways
- Removal of respiratory secretions
- Drug and anesthesia administration
- Cardiopulmonary resuscitation
- To prevent aspiration in unconscious/ comatose patients
- Connected to AMBU bag for mechanical ventilation
- Contraindications:
- Severe airway obstructions
- Laryngeal edema
- Cervical spine injuries
- Advantages:
- Prevent aspiration
- Better fixation
- Less chance of accidental expulsion
- For +ve pressure ventilation
- Disadvantages:
- Provide persistent necrosis
- Complications:
- Airway obstruction
- Stricture formation
- Pressure necrosis
- If it goes inside: collapse of other site
- Infections
- Pneumothorax

- Naso gastric tube
- Indication:
- Diagnostic:
- Upper GI bleeding
- Upper GI obstruction
- Therapeutic:
- Feeding in unconscious patient
- Nasogastric suction in intestinal obstruction
- GI bleeding
- Acute abdomen
- Post operative
- Medication in comatose
- GI wash or lavage in pyloric stenosis
- Non-corrosive poisoning, drug overdose
- Contraindications:
- Corrosive poisoning
- Kerosene oil poisoning
- Complications:
- Rhinitis, pharyngitis, ulcerations in esophagus
- Aspiration pneumonia/death if tube enters trachea
- Blockage of tube
- Perforation of esophagus
- Chance of respiratory tract infections on prolonged intubation

- Bone marrow biopsy needles
- Most common site: posterior superior iliac spine
- Indications:
- Assess marrow cellularity accurately
- To diagnose: aplastic anemia, hypoplastic leukemia, hypoplastic myelodysplatic syndrome
- Lymphoproliferatice disorders
- Myelorpoliferative disorders
- Diagnosis and staging of:
- Non Hodjkin’s lymphoma
- Hodjkin’s lymphoma
- Malignancy
- Metastatic carcinoma
- Stromal changes: fibrosis, necrosis
- Pyrexia of unknown origin
- Amyloidosis
- Metabolic bone diseases
- Contraindications:
- Bleeding disorders
- Complications:
- Hemorrhage
- Pain
- Infection
- Perforation of major vessels

- Bone marrow aspiration needle .
- Q. Most common Site
Sternum
- Indications:
- Diagnostic:
- Hematological malignancy
- ITP
- Aplastic anemia
- Leukemia
- Megaloblastic anemia
- Infections: Kala Azar
- Therapeutic:
- Bone Marrow Transplantation
- Contraindications
- Infection at site
- Bleeding disorders
- Bone Disorders: osteomyelitis, osteogenesis imperfecta

- Biopsy needle (Trucut)
- Contraindications:
- Bleeding disorders
- Overlying skin or peritoneal infections
- Suspected hemangioma of liver
- Indications:
- Suspicious lesions/lump in breast
- Liver biopsy:
- Complications:
- Injury to blood vessels, bile ducts causing hemorrhage, intrahepatic hematoma, hemophilia, bile pigments

- Lumbar Puncture needle / spinal needle
- Level: L2-L3
- Indications:
- Diagnosis of CNS infections
- Spinal anesthesia
- Diagnosis of Guillain-Barré syndrome
- Diagnosis of aplastic anemia
- For intrasosseous infusion
- Contraindications:
- Raised intracranial tension
- Infection at site
- Spinal deformity
- Bleeding disorders
- Subarachnoid hemorrhage

- Nebulizer
- Indications:
- Delivery of bronchodilator drugs – in:
- Acute asthma
- Bronchospasm
- Chest tightness
- Pneumonia
- Atelactasis
- To aid in expectoration- inhalation of hypertonic saline
- Administration of antibiotics and antifungal agents in some resistant chest infections – Cystic fibrosis
- To aid in expectoration- inhalation of hypertonic saline
- Local analgesia- to relieve dyspnea
- Adverse effects:
- Palpitations
- Tremors
- Tachycardia
- Headache
- Nausea
- Bronchospam
- Contraindications:
- Unstable and increased BP
- Cardiac irritability
- Unconscious patients

- Spirometer
- A spirometer is an apparatus for measuring the volume of air inspired and expired by the lungs
- Indications:
- Give exercise to muscles of inspiration and expiration
- Post operative exercise
- Gold standard Dx of COPD
- Dx of: Asthma, Cystic fibrosis, Pulmonary fibrosis
- To screen for lung diseases in smokers, in certain occupational hazards
- To assess pre-operative risk
- To assess health status before beginning strenuous physical activity programs
- Adverse effects:
- Light headedness
- Headache
- Fainting (due to reduce venous return or vasovagal attack)
- Transient urinary incontinence
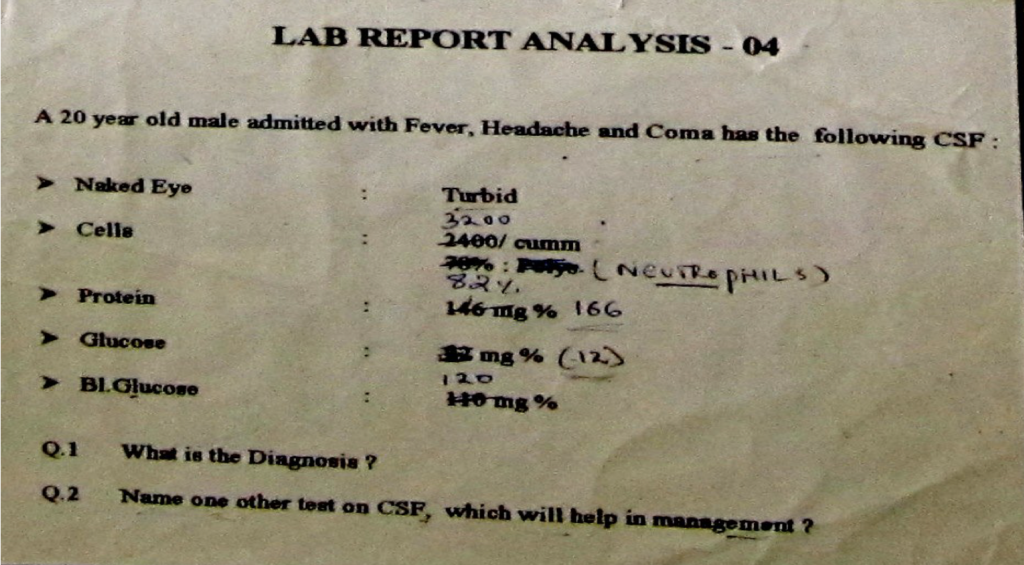
- Pyogenic meningitis
Neutrophils
Low CSF glucose
- CSF culture and sensitivity
Helps in selection of appropriate Abs
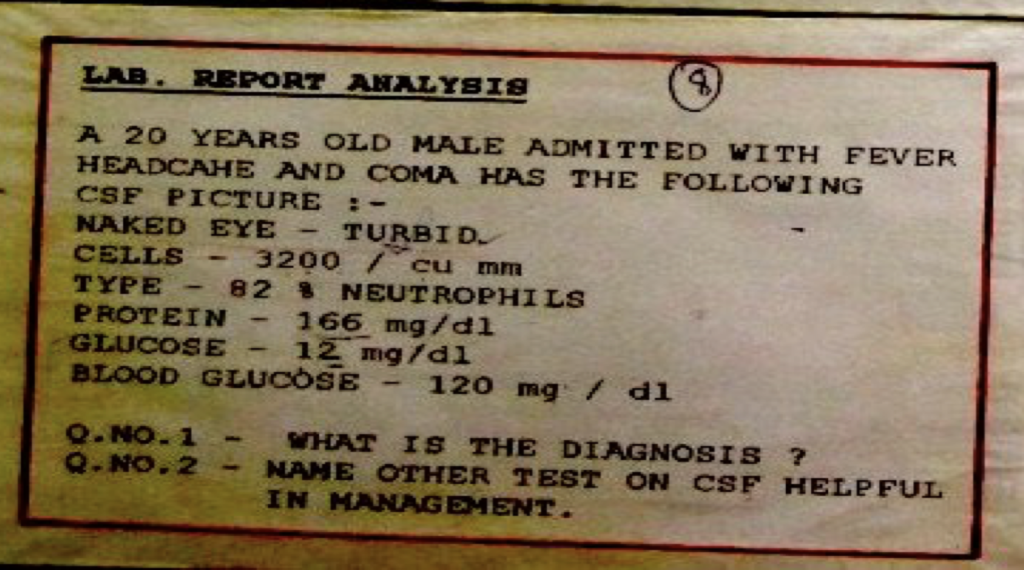
- Pyogenic meningitis
Neutrophils
Low CSF glucose
- CSF culture and sensitivity
Helps in selection of appropriate Abs
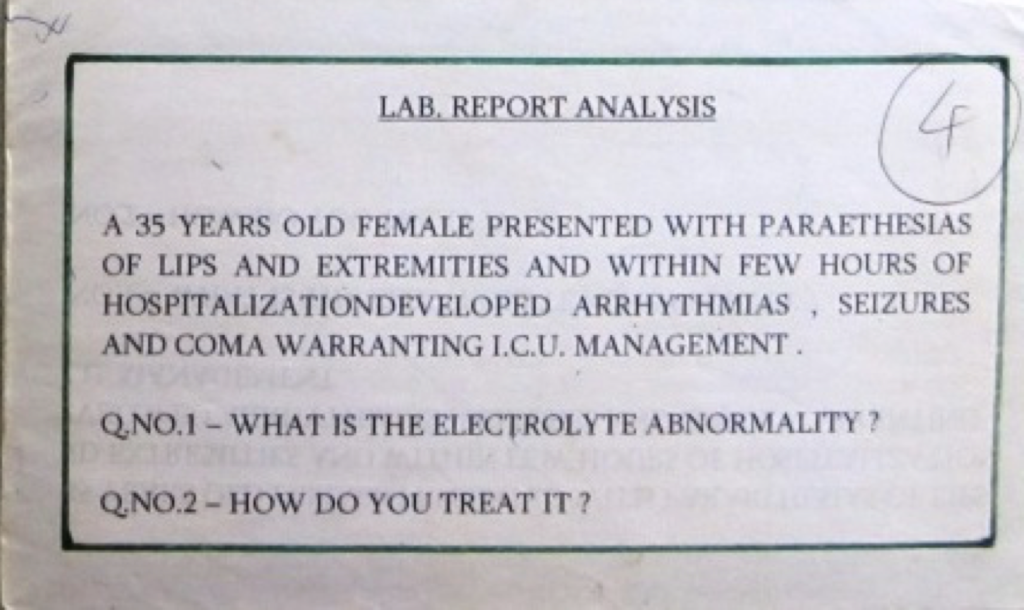
1. Hypocalcemia with tetany
2. 10 ml ( of calcium gluconate 10% by slow intravenous (IV) injection.
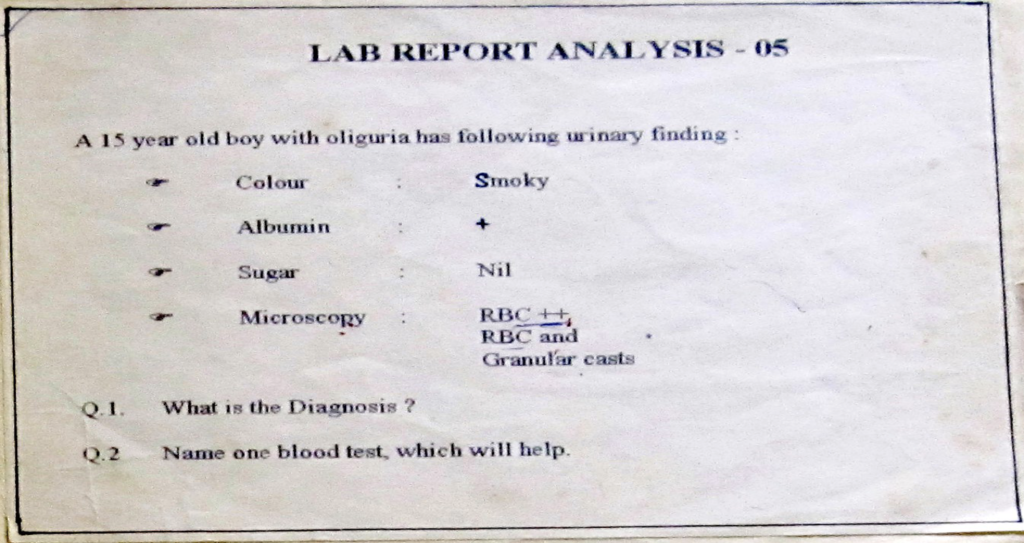
- Nephritic syndrome
Smoky urine,
RBC and cast in microscopy
2. ASO titer, Renal function tests
Urea creatinine – elevation indicates renal impairment
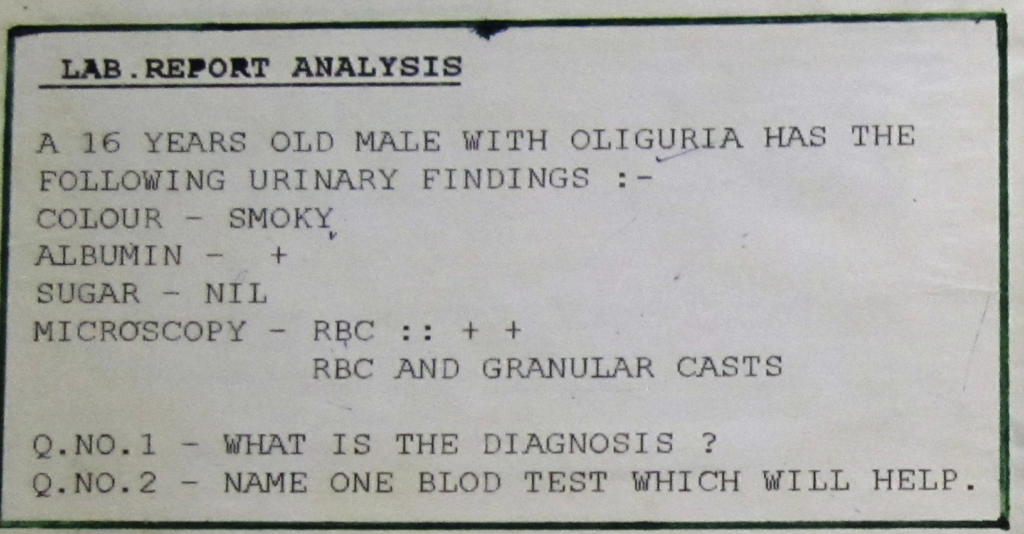
- Nephritic syndrome
Smoky urine,
RBC and cast in microscopy
2. ASO titer
Urea creatinine – elevation indicates renal impairment
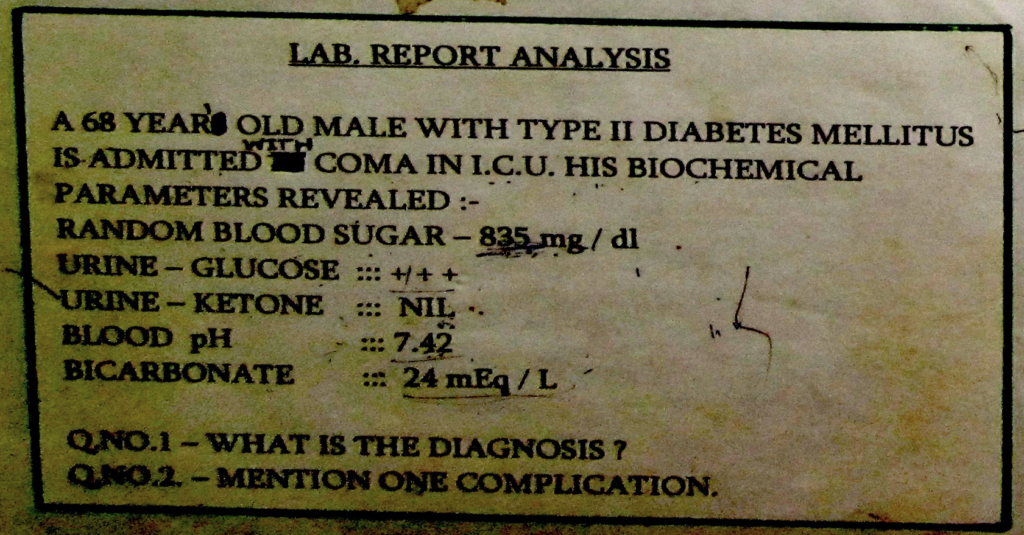
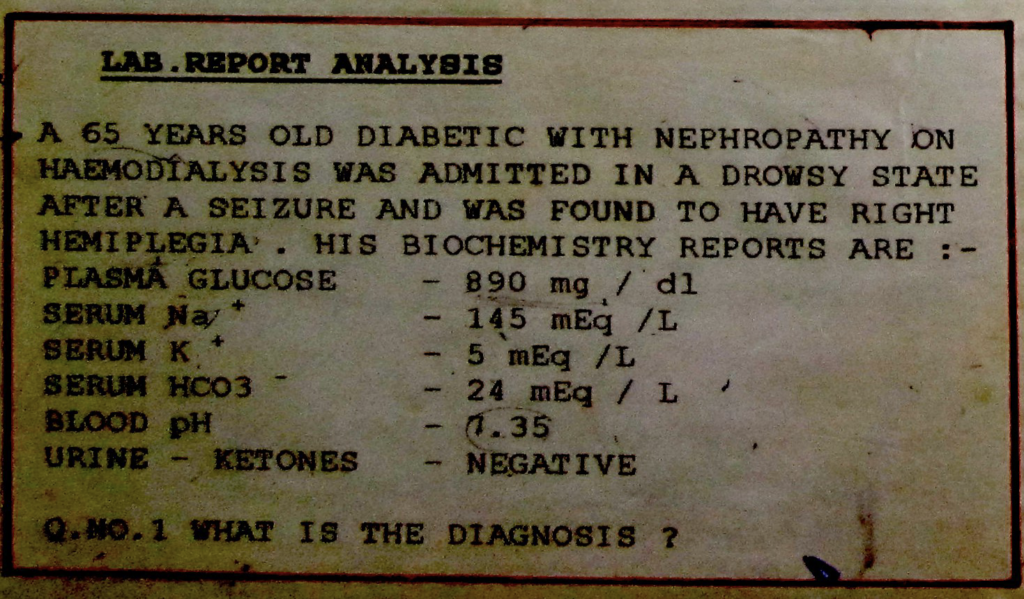
1. Diabetic nonketotic coma ( hyperosmolar nonketotic state, hyperosmolar nonketotic hyperglycaemia)
2. Cerebral infarct
edema
seizures
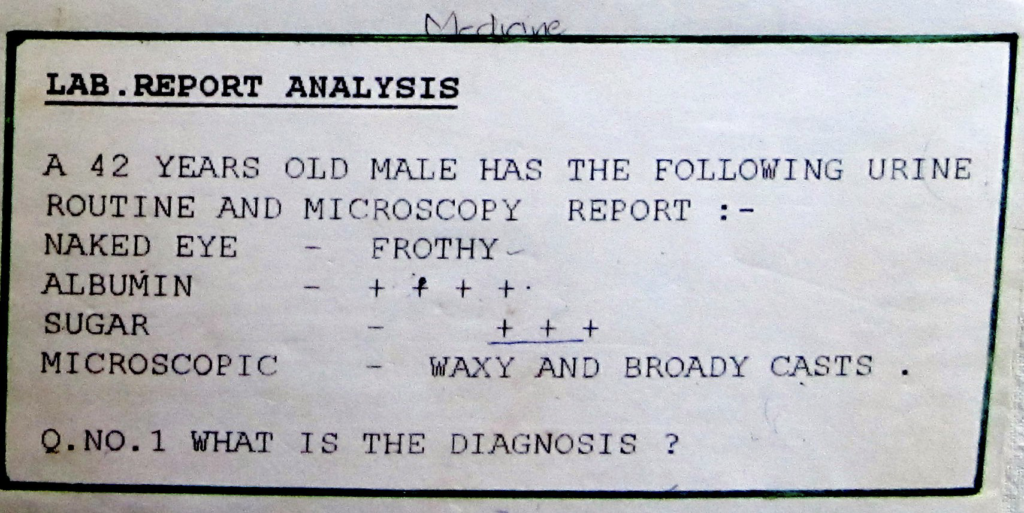
Diabetic nephropathy with nephrotic range proteinuria with chronic renal failure

- Pyelonephritis (upper UTI)
- Urine C/S
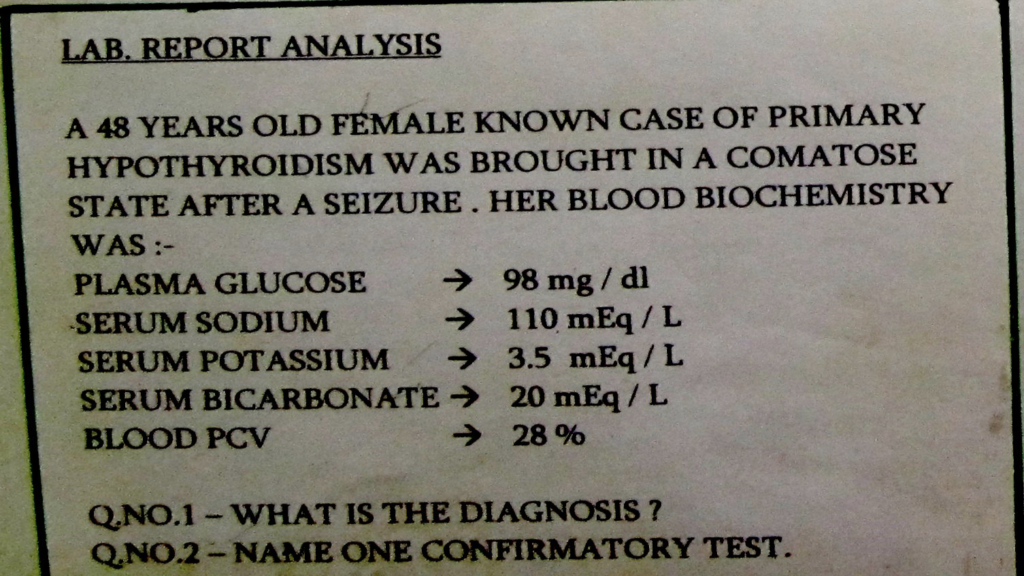
- Myxedema Coma ( known case of hypothyroidism, convulsion, low glucose, Hyponatremia)
- Thyroid function tests
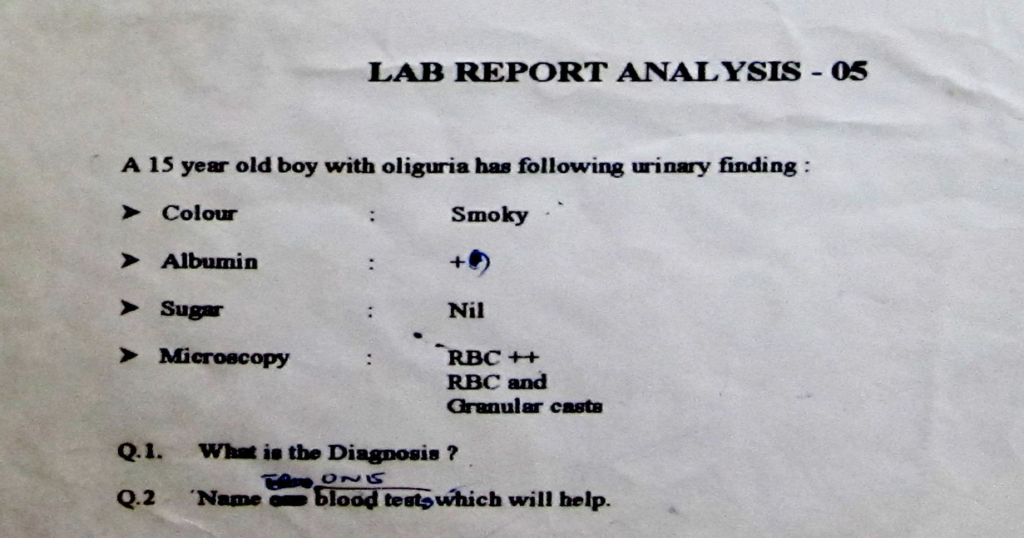
- Nephritic syndrome
Smoky urine,
RBC and cast in microscopy
2. ASO titer, renal function tests
Urea creatinine – elevation indicates renal impairment
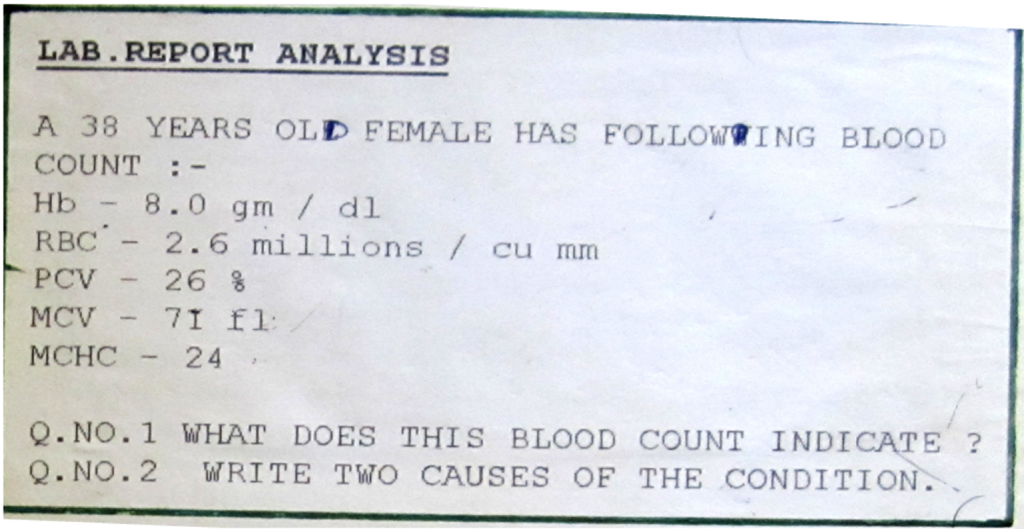
1. Microcytic hypochromic anemia
2. Iron deff & Thalessemia & sideroblastic anemiac anemia
- Diabetic non-ketotic coma ( hyperosmolar non-ketotic state, hyperosmolar
non-ketotic hyperglycaemia)
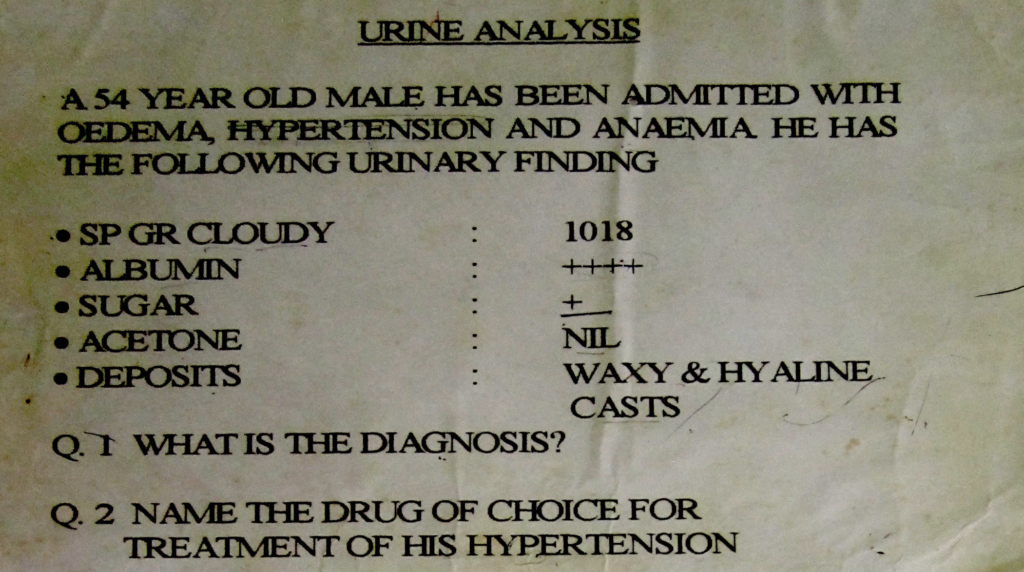
- Diabetic Nephropathy
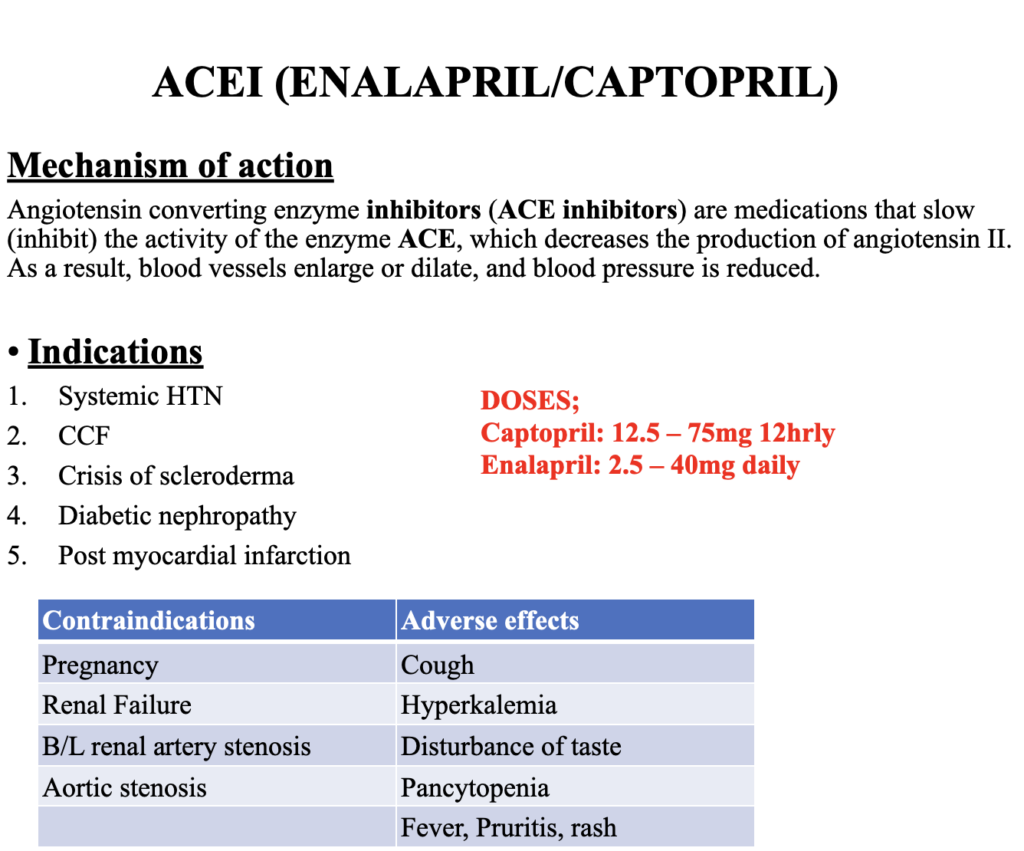
- ACE inhibitors